Prevalence of adenocarcinoma at esophagectomy for Barrett’s esophagus with high grade dysplasia
Division of Gastroenterology, Hepatology & Nutrition, University of Pittsburgh Medical Center, Pittsburgh, PA, USA

|
Original Article
Prevalence of adenocarcinoma at esophagectomy for Barrett’s esophagus with high grade dysplasia
Division of Gastroenterology, Hepatology & Nutrition, University of Pittsburgh Medical Center, Pittsburgh, PA, USA
|
|
Abstract
Background: Barrett’s esophagus with high grade dysplasia (HGD) may require surgical resection because of the risk of concomitant adenocarcinoma. The prevalence of invasive, occult carcinoma (≥stage 1B) in this setting has varied. We investigated the association of adenocarcinoma at operative resection for high grade dysplasia.
Methods: Using an electronic medical record, we identified patients who underwent esophagectomy for high grade dysplasia at the University of Pittsburgh Medical Center between 1993 and 2007. Preoperative diagnosis was confirmed by reviewing endoscopic, radiologic and pathology reports. Postoperative pathology reports were compared to the preoperative diagnosis.
Results: 68 patients (12 females and 56 males) with a preoperative diagnosis of high grade dysplasia underwent operative resection. The mean age was 64 years (range 36 to 86 years). Of 68 patients, 12 (17.6%) had adenocarcinoma, 2 (2.9%) were downgraded to low grade dysplasia, and 54 (79.4%) were confirmed as HGD. Of the 12 patients with adenocarcinoma, 4 (5.9% of total cohort) had intramucosal cancer (Stage 1A) and 8 (11.7% of total cohort) had invasive cancer with submucosal invasion or more advanced disease. Of the 8 patients with invasive adenocarcinoma, 4 did not have preoperative endoscopic or radiologic testing suggestive of advanced disease.
Conclusion: The overall prevalence of adenocarcinoma in association with a preoperative diagnosis of HGD was 17.6%. Invasive adenocarcinoma was present in 11.7% of subjects and was clinically occult in 5.9%.
Key words
Barrett’s, high grade dysplasia, esophagectomy, adenocarcinoma of esophagus
J Gastrointest Oncol 2011; 2: 34-38. DOI: 10.3978/j.issn.2078-6891.2010.027
|
|
Introduction
In Barrett’s esophagus (BE), the esophageal squamous
epithelium undergoes intestinal metaplasia to columnar
mucosa. This transformation has been hypothesized to
occur after prolonged exposure to an acid environment and
is believed to be an intermediate step in the development
of adenocarcinoma. Dysplasia in Barrett’s signif ies
progression toward adenocarcinoma and is classified as
indeterminate, low grade, or high grade dysplasia (HGD). Patients with high grade dysplasia are at higher risk of
developing adenocarcinoma of the esophagus, and may have
concomitant cancer.
Understanding the prevalence of adenocarcinoma in
patients with BE and HGD is critical due to the different
potential approaches to management. Some advocate
surgical treatment as the optimal approach (1-3) while
some favor endoscopic therapeutic treatment (4-7), and
still others prefer to monitor the disease with surveillance
endoscopy to avoid the morbidity and mortality associated
with esophagectomy (8,9).
Several studies have reported on the prevalence of
adenocarcinoma in patients with Barrett’s esophagus
and HGD. In older ser ies, the r isk of concomitant
adenocarcinoma in patients with BE with HGD was as
high as 40% (10). A study of 49 patients who underwent
esophagectomy for HGD reported a cancer incidence of
36.7% (11). More recently, a meta analysis of 23 studies of
patients who underwent esophagectomy for BE and HGD
reported a 12.7% incidence of invasive adenocarcinoma (12). Thus, there has been a wide variation in the prevalence
of adenocarcinoma in patients with BE and HGD.
One factor that may have contributed to this variation
is the differentiation between intramucosal carcinoma and
invasive adenocarcinoma. The esophagus is unique in that
intramucosal cancer does carry a small but definite 3-4%
risk of nodal involvement, but the risk of nodal metastasis
increases to 8 to 33 % with invasive disease, defined as
disease that invades into the submucosa (13). Due to the
difference in risk for nodal metastasis, differentiation of
intramucosal carcinoma from invasive cancer is clinically
important. In the meta-analysis the overall prevalence
of intramucosal and invasive cancer, in a pooled average,
f rom 23 studies was 39.9%. In the 14 studies that
differentiated intramucosal carcinoma from invasive
cancer, the prevalence of invasive cancer was only 12.7%
(12).
The aim of our study was to examine the prevalence of
adenocarcinoma at esophagectomy among patients with a
preoperative endoscopic diagnosis of high grade dysplasia
undergoing surgical resection.
|
|
Methods
Patients were identified through our institution’s medical
record data repository. This repository contains whole-text
medical records and integrates information from central
transcription, laboratory, pharmacy, finance, administrative,
and other departmental databases throughout the University
of Pittsburgh Medical Center hospital system. When
data are imported into the medical archival record system
(MARS), all terms are indexed so that they can be used for
retrieval and cross correlation.
Boolean searches can be executed based on the
mention of any word or combination of words in
admission notes, discharge summaries, radiology reports, and
other documentation.
To meet HIPAA guidelines and insure patient
confidentiality, all data was de-identified using an honest
broker system. This study met the criteria for exemption
of informed consent by the University of Pittsburgh
Institutional Review Board. We identified patients who
underwent esophagectomy for high grade dysplasia in the
setting of Barrett’s esophagus between January 1993 and
June 2007. The search terms used variations of Barrett’s,
high grade dysplasia, adenocarcinoma of esophagus, and
esophagectomy. For inclusion, subjects had to have a preoperative
diagnosis of high grade dysplasia confirmed by
the pathology department at the University of Pittsburgh
Medical Center. Patients with a preoperative diagnosis of
low grade dysplasia or invasive adenocarcinoma or who underwent esophagectomy for other indications were
excluded. Cases were identified by retrospective review
of preoperative pathology reports of biopsy specimens
obtained at endoscopy. After identifying the cohort of
patients undergoing resection, all available preoperative
endoscopy, surgical, and radiology reports for each of the
patients was reviewed.
Postoperative pathology reports were reviewed to
determine whether the final pathologic diagnosis remained
high grade dysplasia, was upgraded to adenocarcinoma, or
was downgraded to low grade or no dysplasia.
In an attempt to provide uniformity in diagnosis of
high grade dysplasia and carcinoma, all preoperative and
postoperative pathology specimens were reviewed by
full time academic pathologist from the Department of
Pathology at the University of Pittsburgh Medical Center.
|
|
Definitions
Intramucosal carcinoma was defined as neoplasia that
invaded into the lamina propria or muscularis mucosa but
not into the submucosal layer. It is considered stage T1a by
the American Joint Committee on Cancer. Invasive cancer
was defined as neoplasia that invaded into the submucosa or
beyond, and is staged as at least T1b.
|
|
Results
A total of 68 patients (12 females and 56 males) underwent
esophagectomy with a preoperative diagnosis of high
grade dysplasia between 1993 and 2007. The mean age
was 64 years (range 36 to 86 years). The average time
between diagnosis of HGD and esophagectomy was 95
days (range 5 to 872 days). Of the 68 patients, on the post
operative specimen, 12 (17.6%) had adenocarcinoma, 2
(2.9%) were downgraded to low grade dysplasia, and 54
(79.4%) were confirmed as HGD. Of the 12 patients with
adenocarcinoma, 4 had intramucosal cancer and 8 had
invasive cancer with submucosal invasion or more advanced
disease (Table 1). Therefore the rate of invasive carcinoma
stage T1b or more was 11.7% (8/68).
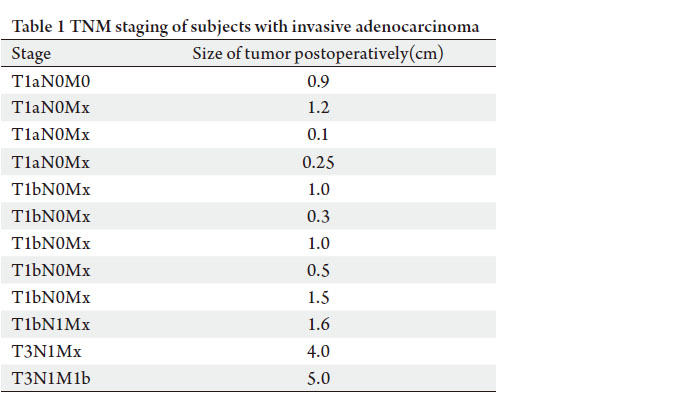
In the 8 patients with a postoperative diagnosis of
invasive cancer, the size of the tumor ranged from 0.3 cm
to 5 cm, with the average 1.86 cm. The TNM staging of
the tumors revealed 5 patients with T1bN0Mx, 1 with
T1bN1M1, 1 with T3N1M1, and 1 with T3N1M0. The 4
patients with intramucosal cancer had tumor sizes ranging
from 0.1 to 1.2 cm, with an average of 0.61 cm.
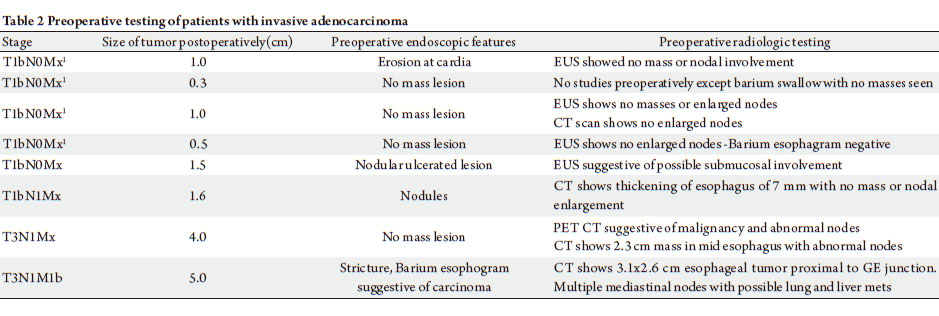
The 2 tumors with T3 staging postoperatively had tumor
sizes of 4 cm and 5 cm. The patient with the 4 cm tumor
had evidence of malignancy on a preoperative positron emission tomography – computerized tomography (CT) scan.
On endoscopic ultrasound, this patient had multiple enlarged
thoracic lymph nodes. The patient with the 5 cm tumor had a
preoperative CT scan revealing a 3.1 cm mass with multiple
mediastinal lymph nodes. This same patient had a preoperative
barium esophogram suggestive of an esophageal stricture. Two
other patients had preoperative findings suggestive of invasive
disease. The patient with a 1.6 cm tumor staged as T1b had
esophageal thickening up to 7 mm noted on a preoperative
computed tomography scan and on preoperative endoscopy
multiple esophageal nodules were noted. The patient with
T1b staging and a 1.5 cm tumor had nodular, ulcerated lesions
on endoscopy and a preoperative endoscopic ultrasound was
suggestive of submucosal involvement (Table 2). None of the
other patients with invasive cancer or intramucosal carcinoma
had radiologic or endoscopic evidence suggestive of cancer on
preoperative testing.
Despite a preoperative diagnosis of HGD 2 patients staged
as T3 had radiologic and endoscopic evidence to suggest
invasive cancer. Two patients with subsequent T1b staging
postoperatively also had preoperative suspicion for malignancy.
Thus, 4 patients with preoperative HGD had occult carcinoma
detected postoperatively, for an occult incidence rate of 5.9%
(4/68).
We performed a time based analysis, based on date of surgical
resection to see if the rate of adenocarcinoma in association with
HGD decreased over time. We divided patients to 2 groups:
those who underwent surgery between 1993 and 2000, and those
between 2000 and 2007. Three of 20 patients (15%) were found
to have adenocarcinoma in first group, while 9 of 48 (18.8%)
were found to have adenocarcinoma in second group (P=0.77).
Even when the groups were analyzed from 1993 to 2003 and
2004 to 2007, no significant difference was found (8/40 and 4/28 respectively, P=0.379).
|
|
Discussion
In this large surgical series examining adenocarcinoma
in Barrett’s esophagus with a preoperative diagnosis of
high grade dysplasia, we report an overall prevalence
of adenocarcinoma of 17.6% with 11.7% invasive and
5.9% occult. This is in contrast to previous early surgical
reports where a much higher rate of adenocarcinoma was
observed. In the meta analysis of 23 studies involving
441 patients undergoing surgery for HGD, the pooled
rate of adenocarcinoma was 39.9% (12). However, in
14 studies within the meta analysis where a distinction
between intramucosal and invasive carcinoma was possible
and the intramucosal cancers were excluded, the rate of
invasive adenocarcinoma fell to 12.7%, consistent with
our observation. In another recent surgical series, the rate
of invasive adenocarcinoma at surgery for HGD was 6.7%
(4/60) (14).
Several predictors of invasive carcinoma in the setting of
HGD have been recognized. Nodular lesions in HGD have
been shown to be at a higher risk for adenocarcinoma (15).
A recent study analyzed pooled data from multiple studies,
and showed that visible lesions at endoscopy are associated
with a higher risk of submucosal invasion, although
statistical significance was not reached (12).
Determining the true rate of occult adenocarcinoma
in Barrett’s with HGD is important because it impacts
on the recommendations for management. If the rate of
malignancy were 40% or even higher, than the associated
risk of mortality to adenocarcinoma would be substantial
enough that surgery would be the optimal choice. However,
if the rate is more on the order of 8% -12%, than the risk of
surgery must be weighed against the risk of the operation,
and the potential response to less invasive treatments such
as endoscopic therapy, including mucosal resection or
photoablative or radioablative treatment. Esophagectomy
is a procedure with a mortality risk of 3% to 8%, and with
risk for significant morbidity, even at the most experienced
centers. In a lower volume center, these risks are higher
(10,16). A recent study from the University of Pittsburgh
reported a 30 day mortality of 0% for T1 cancer patients
undergoing esophagectomy, so local expertise may affect
the clinical approach (17). Multiple patient factors including
patient age and health status must be considered when
deciding on the management of patients with HGD.
A recent review of 1074 patients from 16 studies,
concluded that endoscopic therapy including photodynamic
therapy, argon plasma coagulation, or radiofrequency
ablation, can eradicate Barrett’s disease and dysplasia, and were generally well tolerated (18). It is possible that
endoscopic therapy might have been successful in the 4
patients in our cohort with T1a stage intramucosal disease.
One limitation of our study is the lack of standardized
preoperative testing for the patients in our cohort. A lack of
comprehensive preoperative testing may have contributed
to a higher rate of occult cancer, by increasing patients in
the group with no suspicion for invasive cancer. Three of
the four subjects with occult invasive adenocarcinoma
did not undergo radiologic assessment at our center.
Because of our using deidentified data, we could not rereview
the outside studies. However, these subjects had
very small tumors without lymph node involvement, and
the likelihood that they were truly occult is high. As with
all retrospective studies, selection bias remains a concern,
although we attempted to minimize bias by searching our
electronic medical records using comprehensive inclusion
and exclusion criteria.
The rate of invasive adenocarcinoma in association
with HGD and Barrett’s in this series was 11.7% with 5.9%
having occult adenocarcinoma. When analyzed based on
the date of surgery, we did not find any significant difference
in the rate of detection of postoperative adenocarcinoma in
patients with HGD over time, indicating that rate of cancer
detection did not change in more recent years with the
advent of more modern endoscopic techniques and imaging.
Debate continues as to the best management strategy
when HGD is diagnosed in the setting of Barrett’s esophagus.
Prior studies may have overestimated the risk of invasive
cancer, by inclusion of intramucosal carcinoma, which has
a much lower risk of nodal metastasis. Our study confirms
a low rate of occult cancer in patients with HGD, making
endoscopic therapy an attractive alternative to surgery.
|
|
References
Cite this article as:
Nasr J, Schoen R. Prevalence of adenocarcinoma at esophagectomy for Barrett’s esophagus with high grade dysplasia. J Gastrointest Oncol. 2011;2(1):34-38. DOI:10.3978/j.issn.2078-6891.2010.027
|

