|
Introduction
The treatment of metastatic colorectal cancer (mCRC) has
made significant progress in the past decade, including the
introduction of agents targeting epidermal growth factor
receptor (EGFR). The therapeutic success of monoclonal
antibodies against EGFR (cetuximab and panitumumab)
in treating patients with mCRC highlights the importance
of counteracting the EGFR pathway to control advanced
disease ( 1). In unselected patient populations, response to
anti-EGFR treatment has been modest, which prompted investigators to identify biomarkers that predict increased
likelihood of response in a subpopulation. Among a number
of potential biomarkers studied, mutational activation of
RAS oncogenes has emerged as the most important factor
for determining non-responsiveness to EGFR inhibitors. KRAS is a protein which in humans is encoded by
the KRAS gene and functions as an essential component
of the EGFR signaling cascade. Activating mutations in
KRAS gene cause constitutively active Ras GTPase, which
leads to over-activation of downstream Raf/Erk/Map
kinase and other signaling pathways, resulting in cell
transformation and tumorigenesis (Fig 1) ( 2, 3). KRAS
mutations are present in approximately 30% to 50% of colon
cancer specimens ( 4). Fearon and Vogelstein established a
stepwise hypothesis for colorectal cancer tumorigenesis and
delineated the importance of mutation in RAS gene as an
initiating event in the formation of malignant tumor ( 5). Preclinical studies have suggested that constitutively
activated mutant KRAS can promote tumor invasion and
metastasis by stimulating matrix metalloproteases, cysteine
proteases, serine proteases, and urokinase plasminogen activator that facilitate migration through the basement
membrane ( 6, 7, 8). Despite such findings the role of KRAS
mutation in prognosis of mCRC patients is not clear. The
RASCAL study, which was the largest study designed to
analyze the prognostic value of KRAS status showed that
a glycine-to-valine mutation in codon 12 increased the
likelihood of disease relapse and a lower overall survival
(OS) ( 9). Multiple other studies with smaller sample size
did not demonstrate any impact of KRAS mutations on
survival ( 10, 11, 12). Even in the updated RASCAL II study,
the evidence of a statistically significant worse clinical
outcome was limited to stage III disease and was not
confirmed for other stages ( 13). These results are limited
by their retrospective nature and lack of adequate power to
detect significant differences. The relationship between KRAS status of primary tumor
and stage at diagnosis as well as pattern of spread is also not
clear. Samowitz et al. reported that codon 12 mutations
in KRAS gene were found to be much more common in proximal tumors and were associated with advance stage
at presentation ( 14). Bazan and colleagues showed that
codon 12 mutation in tumor was associated with mucinous
histology and mutation in codon 13 was associated with
advanced Duke stage ( 15). In a retrospective study KRAS
mutation of the primary tumor was also associated with
higher incidence of metastatic disease to lungs ( 16).
Analysis of KRAS and BRAF mutation status in PETACC-3,
an adjuvant trial with 3,278 patients with stage II to III
colon cancer revealed that incidence of either mutation was
not significantly different according to tumor stage. KRAS
mutation was associated with grade of the tumor, while
BRAF mutation was associated with right-sided tumors,
older age, female gender, high grade, and MSI-high tumors.
KRAS mutations were not prognostically related to relapsefree
survival (RFS) or OS whereas BRAF mutation was not
prognostic for RFS, but was for OS, particularly in patients
with microsatellite instability-low (MSI-L) and stable
(MSI-S) tumors ( 17). Multiple studies have demonstrated an association
between KRAS mutational status in the primary tumor
and resistance to EGFR inhibitors (cetux imab and
panitumumab) in patients with mCRC ( 18, 19). Recently
based on convincing data, National Comprehensive Cancer
Network (NCCN) has also made recommendation that
patients with known KRAS mutations should not be treated
with EGFR inhibitors ( 20). Although there is robust data regarding the association
of WT KRAS status and response to EGFR inhibitors,
the relationship between KRAS MT and response to first
line oxaliplatin based chemotherapy without anti-EGFR
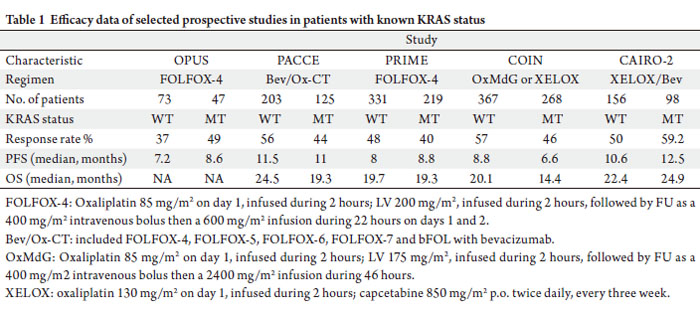
antibodies is conf licting. Two previous first-line studies
showed an improved trend in response rate (RR) and
progression free survival (PFS) in mCRC patients with
KRAS MT, who were treated with first line chemotherapy
regimen including oxaliplatin without cetux imab or
panitumumab while others have reported a worsened
outlook for patients with KRAS MT who were treated
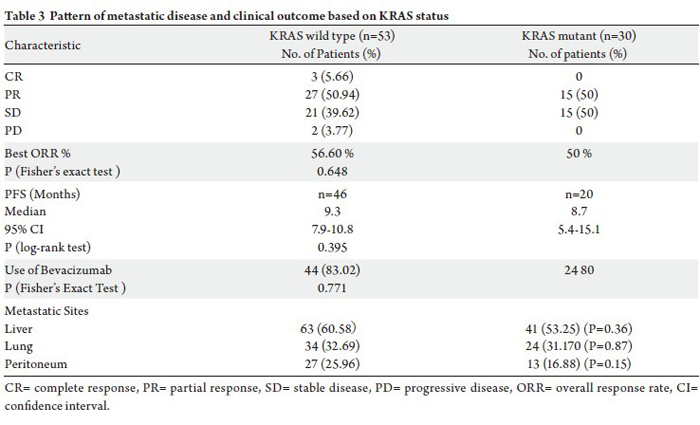
similarly (Table 1) ( 21, 22). In this study, we aimed to address the impact of KRAS
on the pattern of metastatic disease at presentation and on
clinical outcome with first line FOLFOX chemotherapy.
|
|
References
- Van Cutsem E, Kohne CH, Hitre E, Zaluski J, Chang Chien CR,
Makhson A, et al. Cetuximab and chemotherapy as initial treatment for
metastatic colorectal cancer. N Engl J Med 2009;360:1408-17.[LinkOut]
- Wood KW, Sarnecki C, Roberts TM, Blenis J. ras mediates nerve
growth factor receptor modulation of three signal-transducing protein
kinases: MAP kinase, Raf-1, and RSK. Cell 1992;68:1041-50.[LinkOut]
- Leevers SJ, Marshall CJ. Activation of extracellular signal-regulated
kinase, ERK2, by p21ras oncoprotein. EMBO J 1992;11:569-74.[LinkOut]
- Bos JL, Fearon ER, Hamilton SR, Verlaan-de Vries M, van Boom
JH, van der Eb AJ, et al. Prevalence of ras gene mutations in human
colorectal cancers. Nature 1987;327:293-7.[LinkOut]
- Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis.
Cell 1990;61:759-67.[LinkOut]
- Yamamoto H, Itoh F, Senota A, Adachi Y, Yoshimoto M, Endoh T, et
al. Expression of matrix metalloproteinase matrilysin (MMP-7) was
induced by activated Ki-ras via AP-1 activation in SW1417 colon cancer
cells. J Clin Lab Anal 1995;9:297-301.[LinkOut]
- Jankun J, Maher VM, McCormick JJ. Malignant transformation of
human fibroblasts correlates with increased activity of receptor-bound
plasminogen activator. Cancer Res 1991;51:1221-6.[LinkOut]
- Buo L, Meling GI, Karlsrud TS, Johansen HT, Aasen AO. Antigen
levels of urokinase plasminogen activator and its receptor at the tumorhost
interface of colorectal adenocarcinomas are related to tumor
aggressiveness. Hum Pathol 1995;26:1133-8.[LinkOut]
- Andreyev HJ, Norman AR, Cunningham D, Oates JR, Clarke PA.
Kirsten ras mutations in patients with colorectal cancer: the multicenter
"RASCAL" study. J Natl Cancer Inst 1998;90:675-84.[LinkOut]
- Tortola S, Marcuello E, Gonzalez I, Reyes G, Arribas R, Aiza G, et al.
p53 and K-ras gene mutations correlate with tumor aggressiveness but
are not of routine prognostic value in colorectal cancer. J Clin Oncol
1999;17:1375-81.[LinkOut]
- Bell SM, Scott N, Cross D, Sagar P, Lewis FA, Blair GE, et al. Prognostic
value of p53 overexpression and c-Ki-ras gene mutations in colorectal
cancer. Gastroenterology 1993;104:57-64.[LinkOut]
- Dix BR, Robbins P, Soong R, Jenner D, House AK, Iacopetta BJ. The
common molecular genetic alterations in Dukes' B and C colorectal carcinomas are not short-term prognostic indicators of survival. Int J
Cancer 1994;59:747-51.[LinkOut]
- Andreyev HJ, Norman AR, Cunningham D, Oates J, Dix BR, Iacopetta
BJ, et al. Kirsten ras mutations in patients with colorectal cancer: the
'RASCAL II' study. Br J Cancer 2001;85:692-6.[LinkOut]
- Samowitz WS, Curtin K, Schaffer D, Robertson M, Leppert M,
Slattery ML. Relationship of Ki-ras mutations in colon cancers to
tumor location, stage, and survival: a population-based study. Cancer
Epidemiol Biomarkers Prev 2000;9:1193-7.[LinkOut]
- Bazan V, Migliavacca M, Zanna I, Tubiolo C, Grassi N, Latteri MA, et
al. Specific codon 13 K-ras mutations are predictive of clinical outcome
in colorectal cancer patients, whereas codon 12 K-ras mutations are
associated with mucinous histotype. Ann Oncol 2002;13:1438-46.[LinkOut]
- Cejas P, Lopez-Gomez M, Aguayo C, Madero R, de Castro Carpeno
J, Belda-Iniesta C, et al. KRAS mutations in primary colorectal cancer
tumors and related metastases: a potential role in prediction of lung
metastasis. PLoS One 2009;4:e8199.[LinkOut]
- Roth AD, Tejpar S, Delorenzi M, Yan P, Fiocca R, Klingbiel D, et al.
Prognostic role of KRAS and BRAF in stage II and III resected colon
cancer: results of the translational study on the PETACC-3, EORTC
40993, SAKK 60-00 trial. J Clin Oncol 2010;28:466-74.[LinkOut]
- Karapetis CS, Khambata-Ford S, Jonker DJ, O'Callaghan CJ, Tu D,
Tebbutt NC, et al. K-ras mutations and benefit from cetuximab in
advanced colorectal cancer. N Engl J Med 2008;359:1757-65.[LinkOut]
- Amado RG, Wolf M, Peeters M, Van Cutsem E, Siena S, Freeman DJ, et
al. Wild-type KRAS is required for panitumumab efficacy in patients
with metastatic colorectal cancer. J Clin Oncol 2008;26:1626-34.[LinkOut]
- Sharma N, He Q, Sharma RP. Sphingosine kinase activity confers
resistance to apoptosis by fumonisin B1 in human embryonic kidney
(HEK-293) cells. Chem Biol Interact 2004;151:33-42.[LinkOut]
- Bokemeyer C, Bondarenko I, Makhson A, Hartmann JT, Aparicio J,
de Braud F, et al. Fluorouracil, leucovorin, and oxaliplatin with and
without cetuximab in the first-line treatment of metastatic colorectal
cancer. J Clin Oncol 2009;27:663-71.[LinkOut]
- Sharma N, Suzuki H, He Q, Sharma RP. Tumor necrosis factor alphamediated
activation of c-Jun NH(2)-terminal kinase as a mechanism
for fumonisin B(1) induced apoptosis in murine primary hepatocytes. J
Biochem Mol Toxicol 2005;19:359-67.[LinkOut]
- Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford
R, et al. New response evaluation criteria in solid tumours: revised
RECIST guideline (version 1.1). Eur J Cancer 2009;45:228-47.[LinkOut]
- Tol J, Koopman M, Cats A, Rodenburg CJ, Creemers GJ, Schrama
JG, et al. Chemotherapy, bevacizumab, and cetuximab in metastatic
colorectal cancer. N Engl J Med 2009;360:563-72.[LinkOut]
- Ince WL, Jubb AM, Holden SN, Holmgren EB, Tobin P, Sridhar M, et
al. Association of k-ras, b-raf, and p53 status with the treatment effect of
bevacizumab. J Natl Cancer Inst 2005;97:981-9.[LinkOut]
Cite this article as:
Sharma N, Saifo M, Tamaskar I, Bhuvaneswari R, Mashtare T, Fakih M. KRAS status and clinical outcome in metastatic colorectal cancer patients treated with first-line FOLFOX chemotherapy. J Gastrointest Oncol. 2010;1(2):90-96. DOI:10.3978/j.issn.2078-6891.2010.022
|